
What are Pediatric Tibial Tubercle Fractures?
Tibial tubercle fractures are quite rare occurrences that typically affect physically active adolescents between the age of 14 and 17. It is caused by violent tensile forces exerted over the tibial tuberosity (a bulge in the tibial bone) during activities involving sudden contraction of the knee extensors (springing and jumping). A history of Osgood-Schlatter disease in the family may increase susceptibility to tibial tubercle fracture.
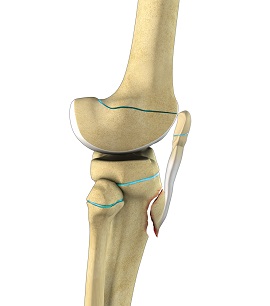
The fractures may occur in three different fashions,
- Type I: Fracture causing a small fragment of bone at the distal end to tear away
- Type II: Fracture occurs at the nearest point to the cartilage bridge, however, the articular surface remains unaffected
- Type III: Fracture line extends into the joint, it is an intra-articular fracture
Tibial tubercle fracture usually occurs during athletic activity and causes symptoms such as pain, swelling over the tibial tuberosity and difficulty in stretching the knee. Type I injuries are mild and the patient may be able to extend the knee away from the ground but may not be able to extend against resistance. In type II and type III injuries, the patient will be unable to extend the knee. The type III injuries may be associated with bleeding into a joint.
Treatment
Type I fractures that are undisplaced are treated by cast immobilization using a long leg cast in full-knee extension. Gradually the patient may be asked to start the rehabilitation of the quadriceps muscles. The other types, type II and III injuries are treated with open reduction and internal fixation followed by cast immobilization for 6-8 weeks. During this procedure, the fracture is reached from an anterior or lateral parapatellar incision. The intervening soft tissue is cleared so that precise reduction of the fracture can take place. In cases of type III injuries, the knee joint is explored for any meniscal and ligamentous damage and arthrotomy may be performed to repair the damaged meniscus. Then the tibial tubercle is reduced and fixed to the tibia with the help of screws. Soon after the procedure, physical therapy and progressive weight-bearing exercises may be initiated.







